TIA - A warning sign
Tips for reducing further risk after a ministroke
Harvard Health Publishing
A transient ischemic attack — TIA — or “ministroke” happens to at least 240,000 people in the United States every year. Symptoms can pass quickly. But that doesn’t mean you should put the episode in the rearview mirror.
A TIA is a warning. Treat it as an opportunity to reduce your risk of going on to develop a full-blown stroke.
What is a TIA?
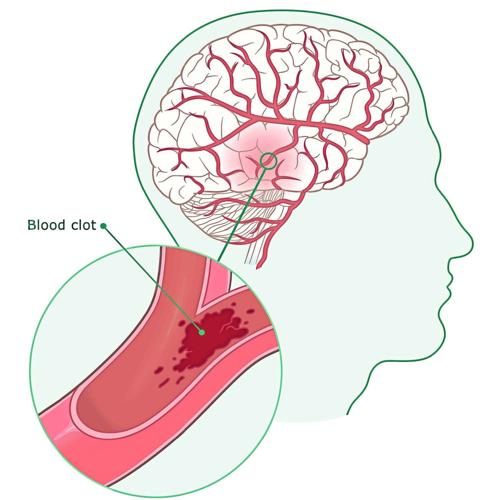
A TIA is a temporary lack of blood flow (and therefore oxygen) in a part of the brain.
It occurs when one or more arteries supplying blood to your brain gets partially or completely blocked, either by plaque or a blood clot. Blood flow usually improves spontaneously within minutes, avoiding permanent brain damage.
Symptoms also are temporary, lasting only a few minutes or hours. The signs come on quickly and are the same as those of a fullblown stroke: sudden face drooping, muscle weakness or numbness on one side of your body, severe headache, confusion and difficulty speaking, seeing or walking.
Because there’s no way to tell in the moment if your symptoms are due to a TIA or a full-blown stroke, always treat it as an emergency. Call 911 to get help right away.
Stroke risk after a TIA
About one-third of those who have a TIA will eventually go on to have a full-blown stroke. The risk is highest during the first 48 hours; up to 10% of people with a TIA go on to have an actual stroke within a couple of days. Your risk of stroke may also be higher if you’re 60 or older and have any of these risk factors:
- Type 2 diabetes.
- High blood pressure.
- Weakness on one side of your body during your TIA.
- Speech problems during your TIA.
- TIA symptoms that lasted for an hour or longer.
- Existing heart disease (severely clogged or narrowed arteries).
Medications after a TIA
It’s not usually necessary to be hospitalized for a TIA. However, it’s likely you’ll be prescribed certain medications to reduce your risk of having a full-blown stroke. An example is antiplatelet drugs that prevent platelets (cell fragments that help blood clot) from clumping together, clogging arteries and raising the risk of a full-blown stroke.
Your doctor may also prescribe medication to treat other underlying conditions that raise your risk of stroke, such as high blood pressure, high cholesterol or a type of irregular heartbeat called atrial fibrillation.
Lifestyle changes can help
Changes in the following areas can help reduce your risk of having a fullblown stroke after a TIA. Taking these steps may feel overwhelming, but they’re worth it, because strokes are often preventable.
1 DIET
A 2021 Harvard study found that eating a plant-based diet rich in foods like leafy greens, whole grains and beans was linked to a reduced overall stroke risk. The Centers for Disease Control and Prevention recommends that you also limit the amount of sodium, or salt, in your diet to lower your blood pressure. Try to avoid or limit foods rich in saturated fat (like full-fat dairy, fried foods and red meat), which raises cholesterol levels.
2 EXERCISE
The CDC recommends all adults get at least 150 minutes per week of moderate intensity aerobic activity (such as brisk walking). If that seems daunting, keep in mind that small bursts of exercise like walking the dog contribute to this overall goal. Try to stay on your feet as much as you can, too. A 2022 study found that sitting more than 13 hours a day was tied to a 44% increased risk for stroke.
3 BLOOD PRESSURE MANAGEMENT
High blood pressure damages the arteries, which can lead to blockages and blood clots. If you’ve had a TIA, it’s important to make sure your blood pressure is under control. Ways to do this include eating a low-salt diet (like the DASH diet), maintaining a healthy weight, exercising regularly, limiting alcohol and not smoking. If your blood pressure is already elevated — at or above a measurement of 130/80 millimeters of mercury (mm Hg) — your doctor may prescribe blood pressure-lowering medication.
4 ADDITIONAL CONSIDERATIONS
It’s also important to follow other healthy lifestyle habits, such as managing stress, controlling your blood sugar levels and weight and getting seven to nine hours of sleep per night.
GLP-1 drugs may fight addiction, new study finds
Tips for reducing further risk after a ministroke
Jonel Aleccia
Associated Press
The blockbuster GLP-1 drugs that reshaped the treatment of diabetes and obesity may help prevent multiple substance use disorders — and reduce their tragic outcomes, a large new study found.
An analysis published this month in the BMJ medical journal looked at electronic health records from more than 600,000 U.S. Veterans Affairs patients with diabetes. It found those treated with medications such as Ozempic and Mounjaro were less likely to develop addictions to substances than those treated with a different class of drugs.
In those already addicted, the GLP-1 drugs were linked to lower risks of hospitalization, overdose and death, according to the study.
The results suggest — but don’t prove — that the weight-loss medications may be able to target the underlying source of cravings that affect the more than 48 million Americans with substance use disorders.
“They’re actually working against the root cause of all these different addictions,” said Dr. Ziyad Al-Aly, the study’s lead author and a chief researcher at the VA St. Louis Health Care System.
What was studied
Previous studies suggested GLP-1s, or glucagon-like peptide-1 receptor agonists, could reduce addictions by targeting the brain’s reward pathways. Those studies were small and often limited to one substance.
For this study, one of the largest to date, Al-Aly and his colleagues analyzed data from the electronic records of more than 600,000 Veterans Affairs patients with diabetes over three years. They compared people who received GLP-1 drugs with those treated with medications that lower blood sugar.
The patients were divided into seven parallel trials that analyzed the risk of developing addictions to multiple substances including alcohol, cannabis, cocaine, nicotine and opioids. Another trial looked at the risk of specific harms among people with existing addictions when they took the different types of medication.
What researchers found
Al-Aly and his colleagues found that people starting the GLP-1 drugs had lower risks of developing addictions. Compared with the other medications, people taking the GLP-1 drugs had a reduced risk for addiction: 18% for alcohol, 14% for cannabis, 20% for both cocaine and nicotine, and 25% for opioids.
In patients who already had substance use disorders, starting the GLP-1s was linked with a 31% lower risk of emergency department visits, 26% lower risk of hospitalizations, 25% lower risk of suicidal thoughts or attempts, 39% lower risk of overdose and 50% lower risk of death.
Overall, the study found use of GLP-1 drugs likely prevented about seven cases of substance use disorder and 12 incidents involving serious harm for every 1,000 users over three years, Al-Aly said.
Limits of the study
Among the study’s limitations: It was conducted within the VA health system, which serves a population that is mostly older, white and male, though Al-Aly said the results were consistent in more than 35,000 women. It also includes data only from people with diabetes, not the general population.
The researchers also couldn’t account for some factors, such as socioeconomic status or lifestyle choices, that could affect the results. The analysis focused on the effects of using GLP-1s compared with another drug, not compared with no treatment.
As an observational study, the new analysis showed GLP-1s are associated with reduced risk of substance use disorders and harms, not that the drugs themselves caused the reduction.
The new findings do not, by themselves, justify prescribing GLP-1 drugs to prevent or treat substance use disorders, Al-Aly said.
That evidence would need to come from randomized controlled clinical trials that directly compare the use of the drugs against a placebo, or dummy medication.
Several such trials are pending, noted Dr. Lorenzo Leggio, a National Institute on Drug Abuse clinical director who wasn’t involved in the study.

Southwest Montana Health Care Directory